When I began this project back in 1980, I knew it was going to be a big job but I had no idea how big. Initially I envisaged it as a three-stage process. Firstly, I planned to do a comparative analysis of a range of modern texts on acupuncture point indications and actions. I chose texts from different parts of China, Taiwan, South Korea, Japan, France, Vietnamese French and USA to afford as broad a range of traditions as possible. The second stage was to explore the historical profile of each indication for each point. As an experiment, I did this with ST 36 (Zusanli) and this eventuated in the paper ‘A Short History of Point Usage: Zusanli’*. This paper took more than a hundred hours to prepare, so it became clear that this was too ambitious a task to undertake for each major point, at least in the short term, so I did not take this any further. Stage Three was going to be an exploration of the modern acupuncture research literature to show which points had been validated as effective for which indications, and what physiological actions were associated with which point. For example, which points were demonstrated to be effective for migraine, and which points had specific physiological actions such as down-regulating Substance P or reducing the expression and sensitivity of TRPV1 receptor.
Now, forty years later I have completed Stage One. While I have attempted to inject some historical and research perspectives into this text, this has only been done at a relatively superficial level, and there is much work still to be done on Stages Two and Three. It is my hope that what I am unable to complete in my lifetime, will perhaps be taken up by other scholars who see value in this project.
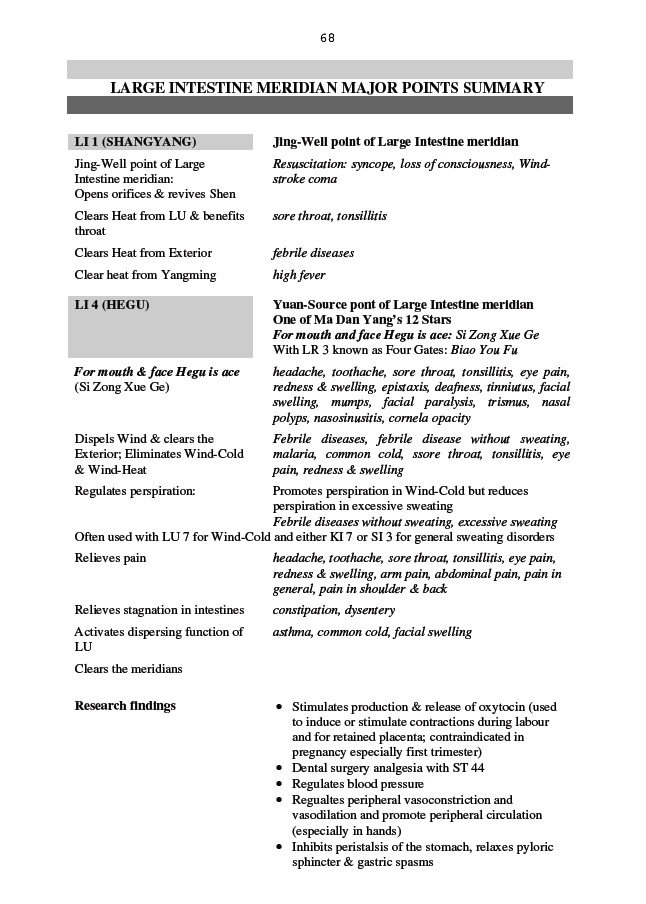
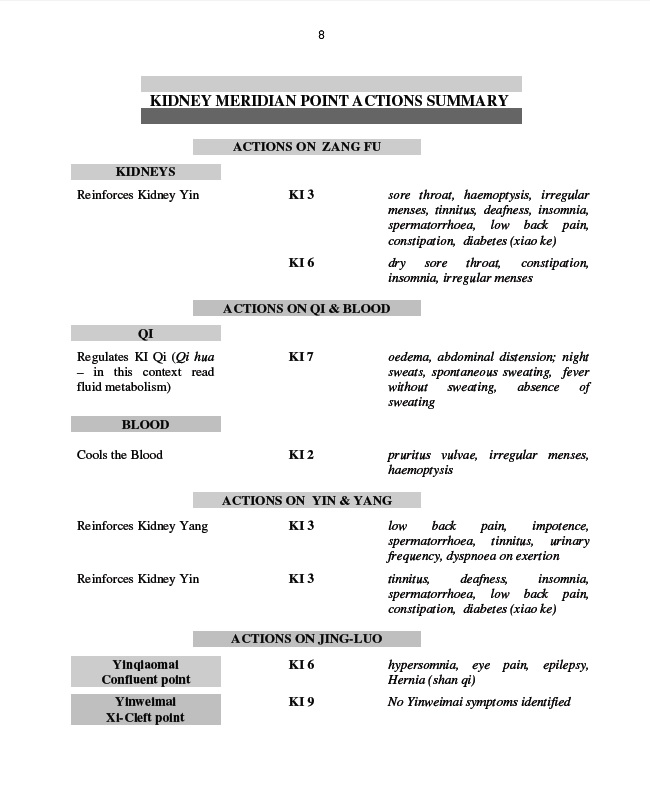
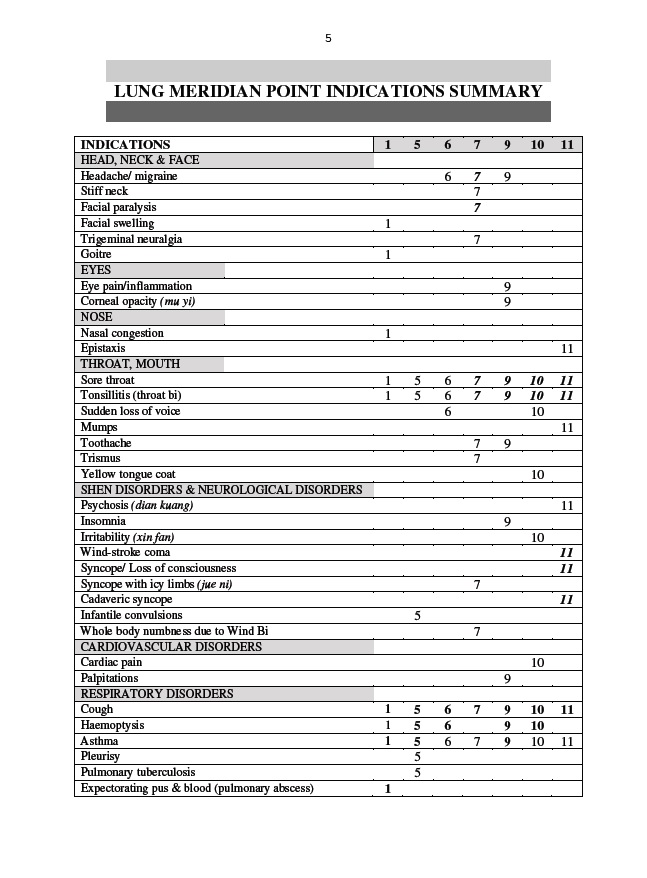
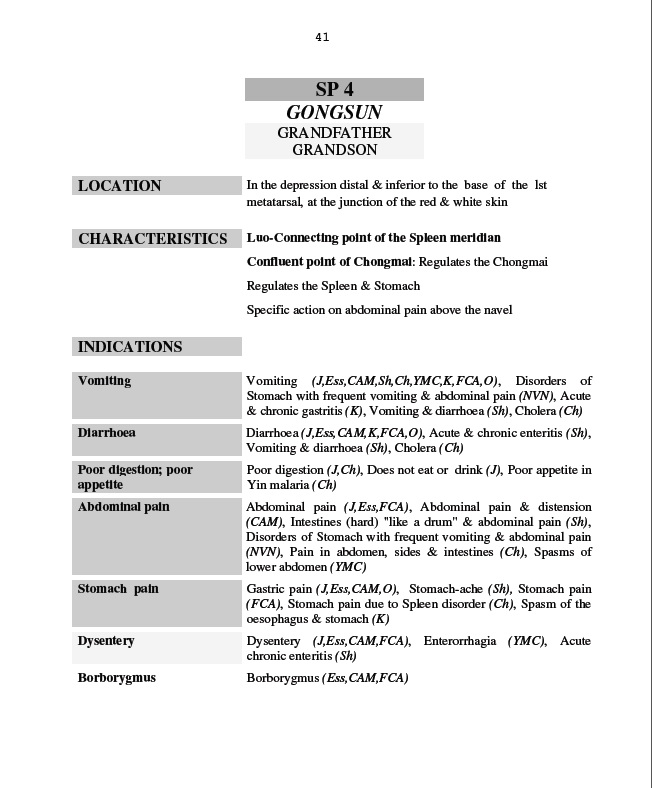
‘Acupuncture Point Dynamics’ (Volumes 1 and 2) is structured in four sections for each meridian – Major Points Summary, Point Indications Summary, Point Actions Summary, Analysis of Major Points. Volume 1 covers the six foot meridians, while Volume 2 covers the six hand meridians, Governing Vessel and Conception Vessel. Here are some sample pages from each section.
References:
*McDonald, J. (1995) A Short History of Point Usage: Zusanli. Pacific Journal of Oriental Medicine, 6:35-44
Anxiety can be very uncomfortable,
even excruciating and paralysing, but Traditional Chinese Medicine has developed
some strategies which might help.
The Yellow Emperor’s Classic of Internal Medicine was a Chinese medical
classic written more than two thousand years ago. This classic introduced the
theory of Five Elements – Wood, Fire, Earth, Metal and Water. The Five Elements
harmonise with each other through the Generating cycle (Sheng cycle) and the Constraining
cycle (Ke cycle).
Wood generates Fire, Fire generates Earth,
Earth generates Metal, Metal generates Water, Water generates Wood.
Wood constrains Earth, Earth constrains Water, Water constrains Fire, Fire constrains Metal, Metal constrains Wood.
The Yellow Emperor’s Classic also associated a particular emotion
with each element – Anger with Wood, Joy with Fire, Reflection with Earth, Grief
with Metal and Fear with Water. The Generating and Constraining relationships
could also be applied to the emotions.
Anger generates Joy, Joy generates
Reflection, Reflection generates Grief, Grief generates Fear, Fear generates
Anger.
Anger constrains Reflection, Reflection constrains Fear, Fear constrains Joy, Joy constrains Grief, Grief constrains Anger.
The Five Element relationships between the emotions was used as
the basis for a therapy by 12th Century Chinese doctor, Zhang Congzheng.
By creating specific emotions, he reasoned that this could generate or constrain
other emotions. Among his case histories he recounts stories of making an emperor
laugh with a comedy performance to break through excessive grief, and provoking
anger to break through excessive reflection. According to Zhang, the Constraining
emotion should be used to produce a short-term effect but for long term
resolution, the Generating emotion should be the focus.
So how can this be applied to dealing
with anxiety? There are several strategies suggested by this model.
Reflection
constrains fear
Fear
is not just a feeling. It is whole body experience. When we experience fear, a
physiological alarm goes off. Our breathing changes, our heart beats faster and
a surge of adrenalin prepares us for fight or flight. But are we reacting to a
real danger, or is it just a perception of danger? Let’s take a scenario of running
late for work on a train. We become anxious and our breathing and heart rate
change. So how big a danger are we really facing here? Let us reflect for a moment.
Are we about to die? No. Suffer serious injury? No. Will our boss physically
attack us when we arrive late to work? Probably not. Will our boss be verbally abusive
and humiliate us in front of the other staff? Probably not. Will we be fired on
the spot? Very unlikely. We arrive at work to find that the boss has not yet
arrived. His train was delayed too. Then we wonder why we agonised through that
entire train journey over a threat which was not real. Reflection can be useful
to assess just how much danger we are really in at any given moment.
Joy
constrains grief, which generates fear
Laughter
helps to move us out of grief, even if only temporarily. These days comedy is
not hard to find and by choosing to watch comedy rather than horror or drama,
we can constrain grief, which in turn will then not generate fear. A good sense
of humour and a hearty laugh can help to move us out of anxiety.
Grief
generates fear
When
fear is a longstanding issue for us, Zhang recommended that we focus on dealing
with our sense of loss. Fear is generated by what we fear to lose. When we have
nothing to lose we have nothing to fear. This is a process which could take a
long time, but there is no rush.
Create
tranquility – breathe
The
opposite of fear is tranquillity. When we are tranquil and serene, anxiety
simply does not arise. The opposite of “fight or flight” is “rest and digest”. When
the sympathetic nervous system is triggered this creates the adrenal rush of “fight
or flight”. The parasympathetic nervous system, when activated, inhibits the sympathetic
nervous system and switches off the alarm – the emergency is past; everything is
fine. This is called the “rest and digest” state. So how do we switch off the
alarm? The key is to deliberately change our breathing. When our breath is
rapid and shallow, our body will believe we are in danger, even if the
emergency is running late for work, as opposed to being in fear of our lives. Our
sympathetic nervous system cannot tell the difference between real danger and anxiety.
The way to switch off the alarm is to breathe like we are perfectly safe –
slowly and deeply. This could be meditation, yoga or Tai Ji Quan but it does
not need to be. We can also achieve the same result by singing or physical activity
(dancing, walking, swimming, exercise) as they all change our breathing. Physical
activity also helps by burning off the arenalin that our body helpfully
provided us with to help us outrun whatever was chasing us.
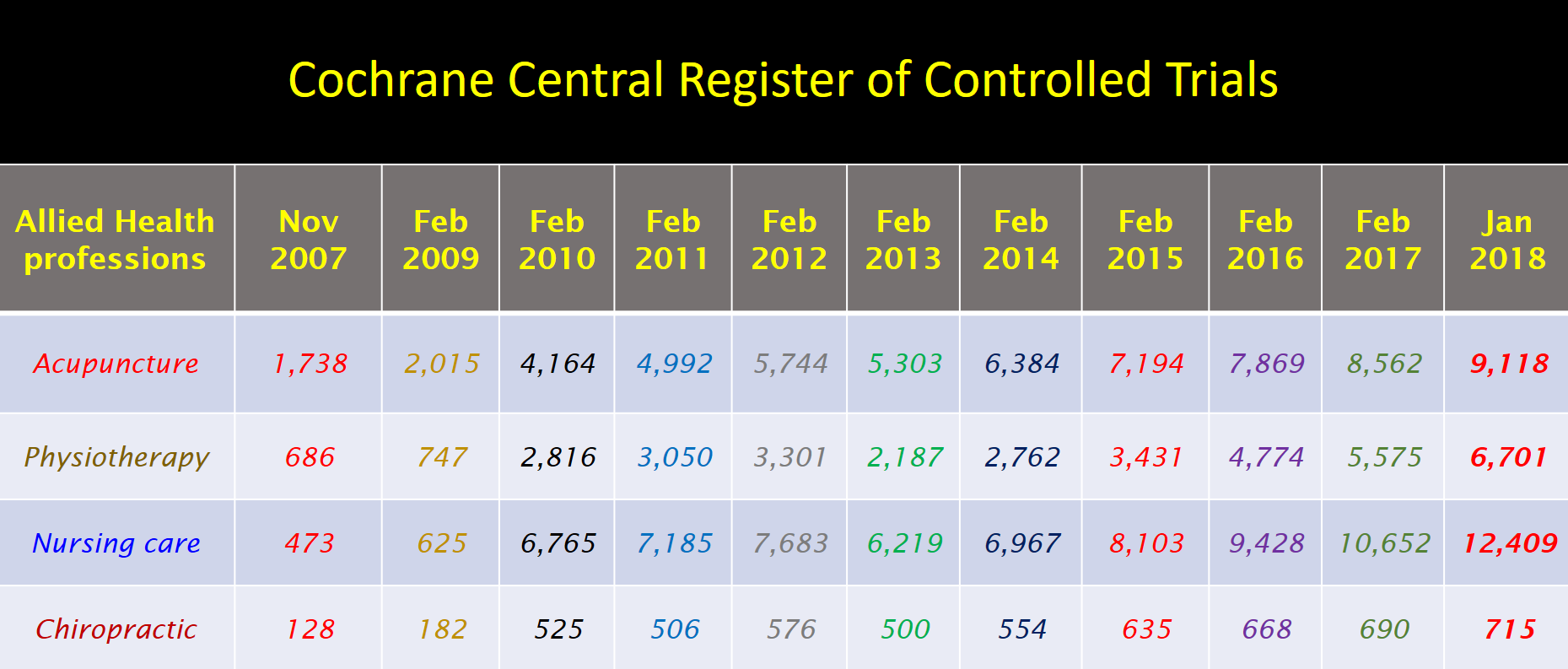
The number of clinical trials investigating acupuncture’s effectiveness and efficacy have now surpassed 9,000 in the Cochrane Register of Clinical Trials. This compares favourably with the number of trials for other Allied Health professions such as physiotherapy and chiropractic, but is unsurprisingly exceeded by nursing research.
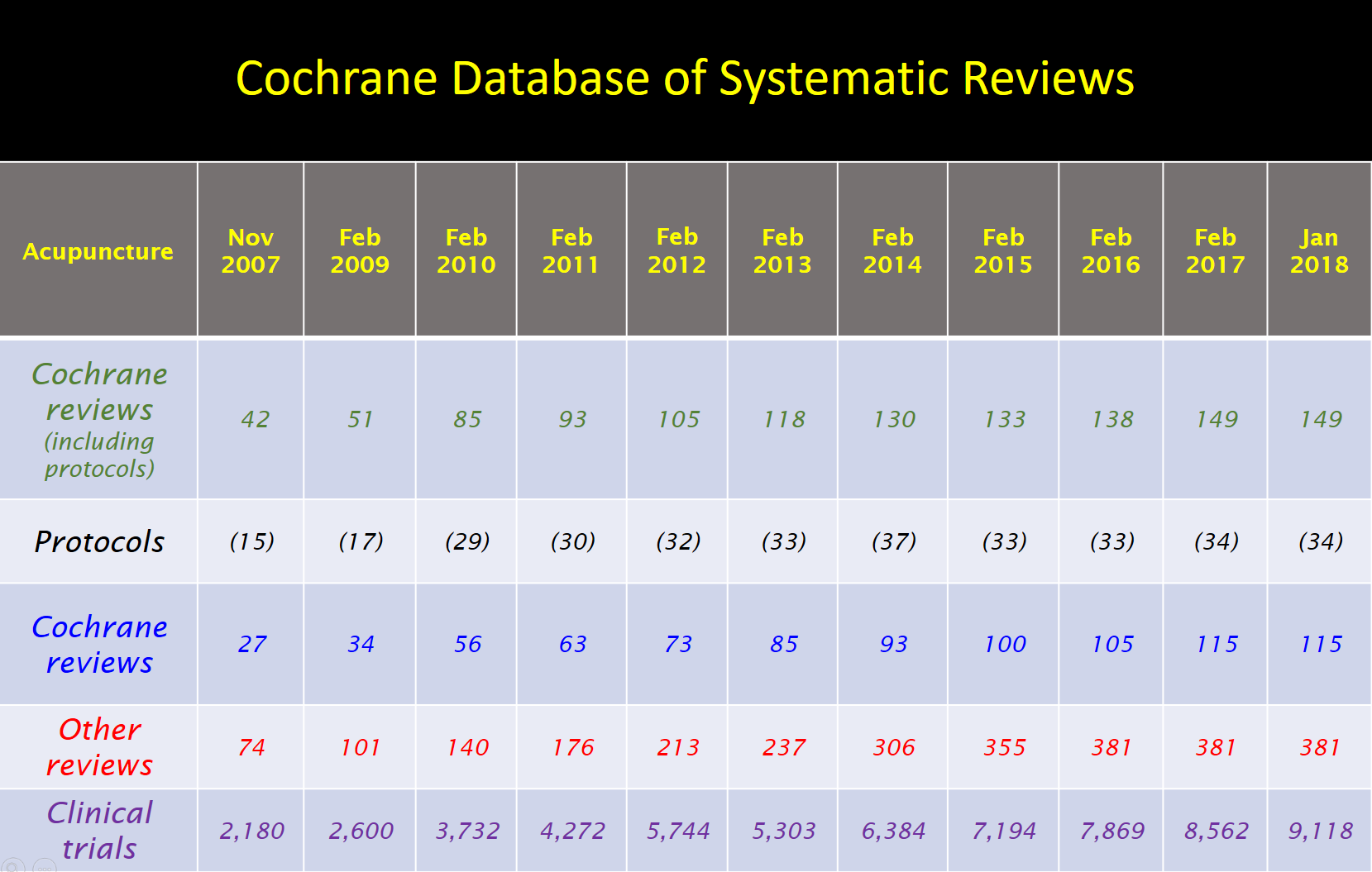
There are also now 115 Cochrane systematic reviews which include acupuncture among other interventions, of which 45 are dedicated solely to acupuncture. There are also an additional 381 systematic reviews on acupuncture published by other reviewers.
The Acupuncture Evidence Project: New review finds mounting evidence
In a new review of acupuncture research, Australian researchers have found that the quality of evidence and the number of conditions for which acupuncture has been shown to be effective has increased significantly since the last major review published by the US Veterans Affairs Department in 2014.
In a project funded by the Australian Acupuncture and Chinese Medicine Association Ltd (AACMA), researcher Dr John McDonald PhD and Stephen Janz reviewed all the systematic reviews of acupuncture published between March 2013, the cut-off date for the US Veterans Affairs ‘Evidence Map of Acupuncture’, and September 2016. A total of 136 systematic reviews, including 27 Cochrane systematic reviews, were included in this review, along with three network meta-analyses, nine reviews of reviews and 20 other reviews. In total over 8,000 randomised controlled trials of acupuncture have now been published and over 1,000 of these were included in the systematic reviews examined. In all, 122 conditions were reviewed.
In the Evidence Map of Acupuncture only three conditions reached the highest level of evidence – ‘Evidence of Positive Effect’. However, that number has risen to eight conditions in the new review: allergic rhinitis; chronic low back pain; migraine prevention; chronic tension-type headache; knee osteoarthritis; post-operative nausea and vomiting; post-operative pain; and chemotherapy-induced nausea and vomiting (CINV).
A further 38 conditions are now graded as ‘Evidence of Potential Positive Effect’ compared to 20 conditions in the 2014 Evidence Map. There was either low quality evidence or conflicting evidence for 71 more conditions categorised as ‘Unclear/ Insufficient evidence’. Only five conditions were found to have ‘No evidence of effect’. In total positive results were found at various levels of evidence for 117 conditions. It is clear that the research effort in acupuncture is accelerating and that many new conditions are now being studied for the first time. The other emerging trend is that researchers are becoming more specific in their research focus. What was once reviewed as just ‘cancer adverse effects’ has now been separated into a dozen different conditions including cancer pain, cancer-related insomnia, cancer-related fatigue, chemotherapy-induced nausea and vomiting.
Where studies on safety or cost-effectiveness of acupuncture were available, these results have been included in the review. Overall, acupuncture was found to safe in the hands of well-trained practitioners, and acupuncture was specifically shown to be safe in treatment of low back pain, migraine, osteoarthritis of the knee, depression, allergic rhinitis, prostatitis pain/chronic pelvic pain syndrome, ambulatory anaesthesia, Alzheimer’s disease and cancer-related psychological symptoms. Studies also showed acupuncture to be cost-effective for low back pain, migraine, headache, chronic pain, neck pain, post-operative nausea and vomiting, osteoarthritis, allergic rhinitis, depression, dysmenorrhoea, ambulatory anaesthesia.
Acupuncture is now recommended by many clinical practice guidelines. By November 2018, 4,552 recommendations for acupuncture were identified for over 300 conditions from multiple international groups and over 30 countries. Examples include:
Non-invasive Treatments for Acute, Sub-acute and Chronic Low Back Pain: A Clinical Practice Guideline from the American College of Physicians 2017
Acute Pain Management: Scientific Evidence published by the Australian and New Zealand College of Anaesthetists and Faculty of Pain Medicine in 2015
Clinical Practice Guidelines for the Management of Rotator Cuff Syndrome in the Workplace published by The University of New South Wales in 2013
Consensus Guidelines for the Management of Postoperative Nausea and Vomiting published in USA by the Society for Ambulatory Anesthesia in 2014
Clinical Practice Guidelines For Allergic Rhinitis published by the Otolaryngology Head Neck Surgery Foundation’s in 2015
TheNational Institute for Health and Care Excellence (NICE), UK for migraine and tension type headache in 2012
Guideline for the Management of Chronic Pain published by The Scottish Intercollegiate Guidelines Network in 2013
Clinical Practice Guidelines for Breast Cancer Treatment published by The National German Gynaecologic Oncology Association’s (Arbeitsgemeinschaft Gynakologische Onkologie) in 2015.
This review reflects the current state of evidence from research, but is not a definition of acupuncture’s scope of practice. When research attempts to validate traditional medical practices which have a history of over two millennia, it takes a great deal of time, research effort and funding to fully explore acupuncture’s scope of practice as it is described anecdotally in the historical literature, which includes thousands of clinical acupuncture books dating from the pre-Christian era to the present day.
What is clear is that the evidence for the effectiveness, safety and cost-effectiveness of acupuncture is growing rapidly.
The Acupuncture Evidence Project by Dr John McDonald, PhD and Stephen Janz was commissioned and funded by the Australian Acupuncture and Chinese Medicine Association Ltd (AACMA).
McDonald J, Janz S. The Acupuncture Evidence Project: A Comparative Literature Review (Revised edition). Brisbane: Australian Acupuncture and Chinese Medicine Association Ltd; 2017.
The full results of our study have now been published in the Annals of Allergy, Asthma and Immunology and Australian Doctor has also reported on our paper.
The purpose of the study, which was conducted at Southport Acupuncture Clinic, Queensland Allergy Services Allergy and Griffith University, was to investigate how the immune system changes in response to acupuncture when treating allergic rhinitis.
The study was funded by the National Health and Medical Research Council and all acupuncture needles for the study were generously donated by Helio Supply Company (Sydney).
I would like to thank all of the 151 allergic and 20 non-allergic volunteers who participated in the study, and all of the research team. Prof Allan Cripps (Pro-Vice-Chancellor Health at Griffith University), Prof Pete Smith (Allergy Specialist and Griffith Professor) and Prof Charlie Xue (Head of Health Sciences at RMIT) were my three supervisors and Associate Professor Caroline Smith (Western Sydney University) and Associate Professor Brenda Golianu (Stanford University) completed our team. I have been most fortunate to have the opportunity, as a first-time researcher, to work with such a wonderful team of people, and to be able to investigate how acupuncture works, a question which has always fascinated me. This study formed the basis of my thesis for Doctor of Philosophy which was awarded on 16th April 2015.
So what did we learn from this study? Firstly, we did see clear evidence that the immune system changes in response to acupuncture and that symptoms continued to improve four weeks after the treatment ceased. In other studies, this improvement has been shown to last for 3 months, and but even at 6 months, although symptoms were starting to deteriorate slightly, they were still much better than before treatment. In clinical practice, a “top up” short course of treatment is therefore recommended if symptoms begin to recur after 3 months.
The symptoms which improved most were nasal congestion, runny nose, sneezing, nasal itch, eye itch and unrefreshed sleep. Post-nasal drip and sinus pain did not improve.
Based on the observation from past studies that all of the studies which used less than 12 treatments and treated less than twice weekly had produced poor or mixed results, whereas all of the studies providing 12 treatments or more, at least twice weekly had been very successful, our study treated twice weekly for 8 weeks. A previous study at RMIT in Melbourne by Prof Charlie Xue and colleagues used twice weekly treatments for 8 weeks rather than 6 weeks so we decided to use the same regimen.
Of those who received real acupuncture in the study, 86.1% of participants showed significant improvements in symptoms and quality of life. Other studies have reported responder rates between 84.6% and 95.8%. Acupuncture treatment has been shown to be very safe with total minor adverse events rate in this study (such as transitory pain on needle insertion or slight bruising) of 3%. Other studies have reported adverse events rates from 0.15% to 4.2%.
In April 2015, the American Academy of Otolaryngology Head and Neck Surgery Foundation updated their Clinical Practice Guidelines for allergic rhinitis in which they recommended acupuncture as a treatment option for patients preferring a non-pharmacologic therapy.
A study in Germany found acupuncture is also cost-effective as a treatment for allergic rhinitis (Witt et al, 2009).
So, in a nutshell, acupuncture is a safe, effective and cost-effective treatment for allergic rhinitis which produces lasting changes in the immune system and hence improvements in symptoms and quality of life.
Dr John McDonald, PhD
McDonald, J.L., Cripps, A.W., Smith, P.K., Smith, C.A., Xue, C.C. & Golianu, B. (2016) Effect of acupuncture on house dust mite specific IgE, substance P, and symptoms in persistent allergic rhinitis Annals of Allergy, Asthma & Immunology (116),6: 497–505
McDonald, J.L., Cripps, A.W., Smith, P.K., Smith, C.A., Xue, C.C. & Golianu, B. (2013) The Anti-inflammatory Effects of Acupuncture and Their Relevance to Allergic Rhinitis: A Narrative Review and Proposed Model. Evidence-Based Complementary and Alternative Medicine, Vol 2013, Article ID 591796.
McDonald, J.L., Cripps, A.W., Smith, P.K. (2015) Mediators, Receptors and Signalling Pathways in the Anti-Inflammatory and Antihyperalgesic Effects of Acupuncture. Evidence-Based Complementary and Alternative Medicine, Vol 2015, Article ID 975632.
The Centres for Disease Control (CDC) in the USA recently called for submissions on their draft revised prescribing guidelines for opioid medications. This was in response to what has been described by the Journal of the American Medical Association as “The Opioid Epidemic” with prescribed opioid medications accounting for more deaths in the US than any illegal drug. The Acupuncture Now Foundation joined with the American Society of Acupuncturists to form the Joint Acupuncture Opioid Task Force which lodged a submission in the CDC process. The main points in the submission were:
Acupuncture is an effective, safe and cost-effective treatment for various types of pain. Acupuncture should be recommended for the treatment of pain before opiates are prescribed.
Acupuncture analgesic mechanisms have been extensively researched and include the production and release of endogenous opioids.
Acupuncture is effective for the treatment of chronic pain involving adverse neuroplasticity.
Acupuncture is a useful adjunctive therapy in opiate dependency and rehabilitation.
Two White Papers regarding the potential role of acupuncture in the opioid crisis have recently been sent to the FDA (Food and Drug Administration) in the US. One was written for the Acupuncture Now Foundation (ANF) by Matthew Bauer and John McDonald, and the second White Paper was a collaboration between ANF and several acupuncture organisations including the American Society of Acupuncturists.